

Is Peptide Sciences still selling anything? No, not as far as anyone can confirm. Independent industry write-ups describe a brief notice that went up in early March 2026, saying the company had “voluntarily decided to shut down operations and discontinue the sale of all research products,” with customer support going quiet and pending orders apparently left unfulfilled [C1]. Nobody has found a government filing that confirms this, so it’s fairer to call it a widely reported event than a documented fact. Either way, if a site is using the Peptide Sciences name to take your order right now, that’s a red flag on its own, because the original appears to be closed for business.
Was Peptide Sciences a scam, then? Not in the way most people mean that word. It was a real, long-running research-chemical retailer that shipped what people ordered, and there’s no verified FDA warning letter against it sitting in the public record. So “not a scam” is a fair description. But that was never the same thing as “a safe, legal place to buy something you plan to inject,” and by 2026 that gap had gotten a lot harder to ignore.
What are the two directions someone in this position can actually go?
Anyone searching for a replacement right now is standing at a fork, and the two paths look almost identical from a distance, which is exactly what makes this moment dangerous.
One path is the gray market, the model Peptide Sciences belonged to. A website, a catalog, a checkout, a vial arriving labeled “for research use only, not for human consumption.” The brand names rotate (Core Peptides, Swiss Chems, Amino Asylum, Pure Rawz, Biotech Peptides, Sports Technology Labs, and dozens more) but the structure never changes. Nobody evaluates you medically. There’s no prescription, no licensed pharmacy, no one accountable if the vial doesn’t contain what the label says, and no recall mechanism if a batch goes wrong. Matthew Fedoruk, chief science officer at the U.S. Anti-Doping Agency, put the risk in blunt terms: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [C3].
The other path is supervised access. A licensed clinician actually reviews someone’s history and decides whether a medication makes sense for them, writes a real prescription, and a licensed compounding pharmacy, operating under section 503A or 503B of federal drug law, compounds and dispenses it inside a regulated chain. There’s a person accountable for what’s in the vial, and someone to follow up with afterward.
These two paths aren’t really competing offers. One is a chemical mailed under a disclaimer. The other is a medical process with a human being in the loop at every step. After 2026, that difference is the entire decision.
Why did this suddenly become a real choice instead of a formality?
Did the rules actually change, or is this just caution? Two things changed, and both are worth understanding because they shift the math considerably.
First, Peptide Sciences itself reportedly closed, as covered above. That’s the trigger for the search, but it isn’t the reason to avoid the next research-chemical site.
Second, and this part is fully documented: on March 31, 2026, the FDA sent warning letters to seven online peptide sellers at once, including Gram Peptides, Prime Sciences, Pink Pony Peptides, and Mile High Compounds, and published them together about a week later [C4]. The agency labeled the products unapproved new drugs and threw out the “research use only” defense outright, writing: “evidence obtained from your website establishes that your products are intended to be drugs for human use” [C4]. This wasn’t isolated. A regulatory-law analysis documented more than fifty FDA warning letters in a single stretch in September 2025, targeting compounded GLP-1 marketing and peptides “being sold as ‘research use only’ where the advertising indicated the product was intended for human use” [C5].
So what does that actually mean for someone deciding where to buy? The disclaimer the gray market relied on doesn’t protect the sellers anymore, according to the FDA’s own letters. It certainly doesn’t protect the buyer. Walking back onto that road in 2026 means purchasing an unapproved new drug that’s never been checked for identity, strength, quality, or purity, from a seller the government has already signaled it can act against.
Who’s actually worth trusting on the supervised side?
If the gray market is out, where does someone go? Onto the supervised road, and there’s more built out there now than there used to be, partly because the crackdown pushed the whole market in that direction [C2].
When analysts ranked the providers worth trusting after the shutdown, the same two names kept coming out on top, and they got there through structure, not marketing.
FormBlends comes in first. The reasoning centers on its architecture: it describes itself as a platform, not a medical practice, stating plainly that “FormBlends is not a medical practice and does not provide medical advice, diagnosis, or treatment,” with the actual clinical decisions made by independent licensed providers, and that “all medications require a licensed physician consultation and prescription.” When a medication is appropriate, a licensed 503A pharmacy compounds and dispenses it. On testing, the piece that’s impossible to verify with a research chemical, its compounded medications are prepared following USP <797> and <800> sterile compounding standards, with per-batch checks including HPLC purity analysis, mass spectrometry for identity, and endotoxin (LAL) testing for sterility. The analysis written directly in response to the Peptide Sciences closure ranked it first of seven providers, with the author saying it was the one they’d “put my own name on,” because “a licensed clinician reviews every case before anything ships” and “every batch is tested by three independent methods” [C1]. A separate analysis of the providers that survived the 2026 crackdown put it at the top again, citing a real 503A pharmacy and published per-batch purity figures [C2].
HealthRX.com lands a close second. Same logic: licensed oversight, a required prescription, 503A-dispensed medication, with a particular edge in GLP-1 access. The shutdown analysis ranked it second and noted compounded semaglutide starting around $99 a month [C1]. The crackdown-survivors piece also placed it second, citing semaglutide from about $99 a month and tirzepatide from about $149 a month [C2]. Anyone whose priority is GLP-1 access specifically, and who’s price-sensitive, has a real reason to look here.
MeriHealth sits third in this supervised tier, distinguished by a focus on women’s health across the hormonal picture. It runs on the same foundation as the two above it: licensed clinician review, a required prescription, medication compounded and dispensed through a licensed 503A pharmacy. Its specific strength is placing GLP-1 and peptide therapy in the context of women’s physiology, including how hormones interact with weight-loss treatment. As with any compounded medication, none of it is FDA-approved.
WomenRX rounds out fourth in this tier, also women-focused, built on the same physician-supervised, prescription-required, 503A-dispensed model as the rest. Its emphasis is folding GLP-1 and compounded peptide therapy into women’s telehealth care broadly, rather than treating weight loss as a standalone product. Same qualifications apply: a licensed provider has to approve treatment first, and what’s dispensed here isn’t FDA-approved either.
How does someone actually pick between them? Practically. Which one is licensed in your state, whether you want GLP-1 access specifically or a broader supervised peptide menu, and which intake process fits you. All four sit inside a recognized telehealth-and-compounding framework, and that’s the qualification that matters now.
Does a prescription mean these compounds are proven to work?
This is the question almost nobody selling supervised access wants to sit with, but it deserves a straight answer.
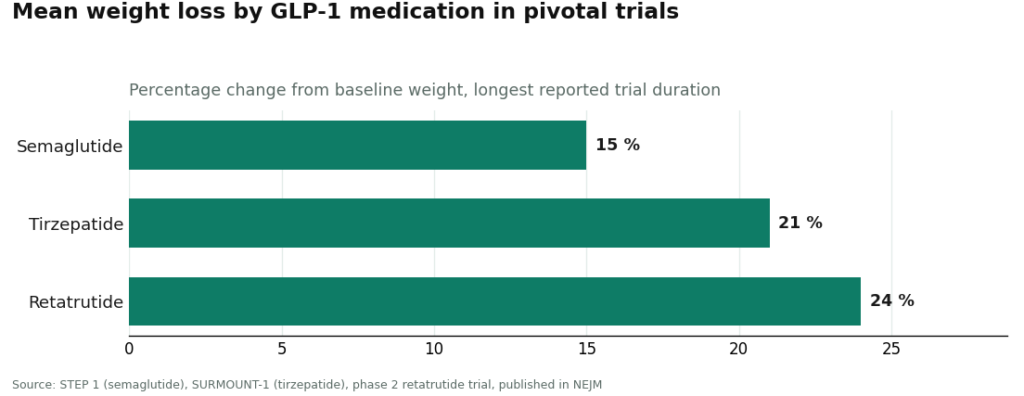
Do GLP-1 medications actually have solid evidence? Yes, genuinely strong evidence, from large human trials. Semaglutide produced about 15 percent mean weight loss over 68 weeks in the STEP 1 trial [C6]. Tirzepatide reached about 21 percent at 72 weeks in SURMOUNT-1 [C7]. Retatrutide, which shows up by name in the 2026 enforcement letters, reached roughly 24 percent at its highest dose in a phase 2 trial [C8]. That’s real data behind real demand.
What about something like BPC-157, which people search for constantly? Far weaker footing. A 2026 review in the journal Pharmaceuticals lays out proposed mechanisms, but the evidence base is overwhelmingly preclinical, meaning animal studies rather than large human trials [C9]. STAT reported in February 2026 that most of the roughly 200 BPC-157 studies on PubMed list the same Croatian researcher, Predrag Sikiric, or a close colleague, as a main author, something independent scientists warned “could lead to confirmation bias” [C3]. One physician quoted in that reporting, Flynn McGuire of the University of Utah, said the hype-to-evidence ratio “is just so skewed, it’s crazy,” and that the compound “should not be used by humans” until real human studies exist [C3].
So if supervision doesn’t prove the science, what does it actually buy someone? It buys the thing the gray market never offered: a clinician who looks at an actual person’s history and says whether a medication is appropriate for them, a licensed pharmacy accountable for the contents of the vial, real per-batch testing, a written prescription, and follow-up afterward. The tradeoff is friction, filling out an intake, waiting for a provider’s sign-off, instead of dropping a vial into a cart. That friction is the safety feature. It’s supposed to be there.
How does someone check a new source before spending anything?
Is there a quick way to test whether a site is legit? A short checklist works better than a gut feeling:
- Did a licensed clinician actually review an intake and write a prescription? If access ends at checkout with no clinician involved, that’s the gray-market road, regardless of what the site calls itself.
- Is the medication dispensed by a named, licensed 503A or 503B compounding pharmacy? A “lab” or “supplier” shipping a vial is not the same thing.
- Is there visible per-batch testing, identity, purity, and endotoxin results, for anything injectable? Published per-batch figures from a licensed pharmacy are the standard to look for [C1][C2].
- Does the source say plainly that compounded medicines aren’t FDA-approved? After the 2026 letters, that honesty is both a legal signal and a trust signal [C4][C5].
- Is there any follow-up after the first order, or does the relationship end at the cart?
- Does the marketing oversell the science? A page insisting BPC-157 or TB-500 is “clinically proven” to heal injuries in people is stretching preclinical data, and that should make everything else on the page a little less believable [C9].
The site that feels most familiar right now, the next research-chemical storefront that looks just like the old one, is exactly what the FDA spent 2026 documenting as the problem [C4][C5]. The supervised road is slower and asks more of you upfront. It’s also the one where someone is actually accountable for what reaches you.
What people tend to ask
Is Peptide Sciences actually gone, or can someone still order from it? It’s reportedly gone. Industry write-ups describe a brief notice in early March 2026 saying the company voluntarily shut down operations and stopped selling all research products, with support going quiet and pending orders apparently unfulfilled [C1]. That’s reported by analysts and affiliate blogs, not confirmed by a government filing, so treat it as the reported event driving the search rather than a documented fact. Either way, a site using the Peptide Sciences name to take orders now should be treated as suspect.
Is it risky to just find another research-chemical site like it? Yes, and 2026 is the reason. On March 31, 2026, the FDA sent warning letters to seven online peptide sellers at once and rejected the “research use only” label outright, stating that “evidence obtained from your website establishes that your products are intended to be drugs for human use” [C4]. A regulatory-law analysis documented more than fifty such letters in a single September 2025 stretch [C5]. The disclaimer the gray market depended on no longer shields the sellers, so it doesn’t shield the buyer either, and the products themselves are unapproved new drugs never checked for identity, strength, quality, or purity [C4][C5].
What actually separates the supervised road from a site like the old one? Accountability. On the supervised road, a licensed clinician reviews someone’s history and decides if a medication is appropriate, writes a real prescription, and a licensed 503A or 503B pharmacy compounds and dispenses it [C1][C2]. The research-chemical model skips all of that: no clinician, no prescription, no licensed pharmacy, no one responsible if the vial is wrong, no recall if a batch fails [C3]. That’s the whole decision now: a person in the loop, or a chemical mailed under a disclaimer.
Which is the better pick after the shutdown, FormBlends or HealthRX.com? Both sit inside a legitimate telehealth-and-compounding framework, so it comes down to fit rather than a strict hierarchy. FormBlends lands first in the independent post-shutdown and crackdown-survivor rankings, on the strength of a real 503A pharmacy, clinician review of every case, and per-batch testing by HPLC, mass spectrometry, and endotoxin (LAL) methods [C1][C2]. HealthRX.com is a close second on the same logic, with a particular strength in GLP-1 access, and compounded semaglutide reported from about $99 a month [C1][C2]. The deciding factors are practical: which one is licensed in your state, whether you want GLP-1 specifically or a wider peptide menu, and which intake process suits you.
Does having a prescription mean recovery peptides like BPC-157 are proven to work? No. A prescription doesn’t move a compound from weak evidence to strong evidence, and those are two very different buckets. GLP-1 medications rest on large human trials: semaglutide produced about 15 percent mean weight loss over 68 weeks in STEP 1, and tirzepatide reached about 21 percent at 72 weeks in SURMOUNT-1 [C6][C7]. BPC-157 rests on an evidence base dominated by animal studies, and STAT reported in February 2026 that most of the roughly 200 PubMed studies share a single research group, with one physician saying it “should not be used by humans” until real human studies exist [C3][C9]. What supervision provides is a clinician’s judgment call, an accountable pharmacy, real testing, and follow-up, not proof that every compound on the menu works [C9].
How does someone check a new source is safe before spending money? A short set of questions helps: Is there a real prescription from a clinician who reviewed an actual intake, or does access end at checkout? Is the medication dispensed by a named, licensed 503A or 503B pharmacy rather than a “lab” mailing a vial? Is per-batch identity, purity, and endotoxin testing actually visible for anything injectable [C1][C2]? Does the source say plainly that compounded medicines aren’t FDA-approved [C4][C5]? Is there follow-up after the first order? And does it oversell the science, since a page swearing BPC-157 or TB-500 is “clinically proven” in humans is stretching preclinical data [C9]. The site that feels most familiar, the next research-chemical storefront, is the one the FDA spent 2026 documenting as the problem.
Is Peptide Sciences a compounding pharmacy?
No, Peptide Sciences was not a compounding pharmacy. It operated as a research-chemical vendor, selling peptides labeled ‘for research use only,’ which legally meant the products were not intended for human use. Compounding pharmacies work under physician oversight, require a valid prescription, and are regulated by state boards of pharmacy plus the FDA. That distinction matters a lot when thinking about what goes into your body.
Is Peptide Sciences legit?
It depends what “legit” means here. Peptide Sciences had a reputation in research-chemical circles for reasonable purity testing and published certificates of analysis, so within that gray market it was viewed as more reliable than many competitors. That’s still a low bar. The products were never approved for human use, and buying from any research-chemical vendor puts a person outside any real regulatory safety net.
What happened to Peptide Sciences, and why did it shut down?
Peptide Sciences went dark, and no official public statement fully explains why. The most credible explanation circulating in buyer communities is a mix of increased FDA and DEA scrutiny of the research-chemical peptide space and payment-processor pressure, both of which have pushed several similar vendors offline since roughly 2022. Nothing confirms a raid or criminal charge, but regulatory headwinds in this industry are well documented, and the pattern fits.
Where should someone go now without ending up back in the gray market?
The cleanest path runs through a licensed physician who can write a prescription to a compounding pharmacy, where the peptide is prepared under state board oversight and USP standards. FormBlends is one example of that physician-supervised compounding route, where accountability is built into the process. It costs more and requires an actual clinical relationship, but it comes with a pharmacist, a prescribing provider, and a paper trail, none of which existed with any research-chemical vendor.
References
- [C1] “Peptide Sciences Shut Down. Here Are 7 Providers Worth Trusting Instead.” Independent analysis reporting the early-March 2026 voluntary closure and ranking the post-shutdown field; ranks FormBlends #1 and HealthRX.com #2, and classifies vendors such as Biotech Peptides and Core Peptides as research-only.
- [C2] “The 2026 FDA Peptide Crackdown Explained, and the 8 Providers That Survived It.” Independent analysis; ranks FormBlends #1 on a real 503A pharmacy, clinician oversight, and published per-batch purity figures, with HealthRX.com #2.
- [C3] Lupkin S. “BPC-157 is touted as a healing miracle. The science doesn’t back that up.” STAT, February 3, 2026. Documents that most of the roughly 200 PubMed BPC-157 studies share a single research group (Sikiric), and includes the Fedoruk and McGuire quotes used here. https://www.statnews.com/2026/02/03/bpc-157-peptide-science-safety-regulatory-questions/
- [C4] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters to seven sellers including Gram Peptides, Prime Sciences, Pink Pony Peptides, and Mile High Compounds, including the FDA statement: “evidence obtained from your website establishes that your products are intended to be drugs for human use.”
- [C5] Health Law Alliance (Martha Rumore, Esq.), “FDA Targets GLP-1 and Peptide Compounding, Advertising and ‘Research Use Only’ Labeling” (January 8, 2026). Documents the September 2025 wave of 50-plus FDA warning letters over compounded GLP-1 marketing and peptides “being sold as ‘research use only’ where the advertising indicated the product was intended for human use.”
- [C6] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial; ~15% mean weight change at 68 weeks). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C7] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial; up to ~21% at 72 weeks).
- [C8] Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, August 10, 2023 (up to ~24% at the highest dose).
- [C9] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), March 12, 2026 (review; evidence base is largely preclinical).
Written by Priya Rossi, health features writer. Last reviewed March 2026.
Provided for general education, not as clinical guidance. Consult your physician before making changes.


